The Swedish Institute for Health Economics (IHE) recently released a new study on cancer care in the MEA Region. The report projects that cancer cases in the region are set to double by 2040. Here are the key highlights from the study.
Cancer around the globe
Globally, millions are already living with a cancer diagnosis. Despite medical advances globally and improvements in diagnosis and treatment, the disease continues to be a challenge around the world. Indeed, the Union for International Cancer Control (UICC), statistics confirm there are around 43.8 million people around the world who are within five years of a cancer diagnosis. It’s alarming, to say the least!
MEA is at risk of more cancer cases
To raise awareness on World Cancer Day, the Swedish Institute for Health Economics (IHE) released a new report that studies cancer care in the MEA Region. Titled ‘Cancer Care in the Middle East and Africa‘, the IHE’s report focuses on nine territories. They are within the MEA-9 region. These include Algeria, Egypt, Jordan, Kuwait, Lebanon. As well as Morocco, Saudi Arabia, South Africa, and the United Arab Emirates (UAE).
Thomas Hofmarcher, Health Economist at IHE explained that“This year’s World Cancer Day included a three-year campaign titled: ‘Close the Care Gap.” The focus is on understanding and recognizing that there are global inequities in cancer care.”
Key factors in MEA that fuel cancer cases
The study has highlighted many concerns. Some of which include demographic changes as well as the continued impact of smoking, obesity, Hepatitis C, HPV, and HIV/AIDs among other issues.
In MEA-9, the annual number of newly diagnosed cancer cases per 100,000 inhabitants has been on the rise since the year 2000. This is attributed to demographic changes, plus an increase in risk factors, such as smoking and obesity.
Due to demographic development, newly diagnosed cancer cases could double from 410,000 to 720,000 cases per year from 2020 to 2040.

sirtravelalot/shutterstock
The Impact of cancer in MEA 9 countries
The IHE hopes this study will raise awareness of the magnitude of the burden of cancer and the need to address the disease comprehensively.
The impact of cancer for the MEA 9 countries in the IHE study is immense and growing. The disease was the third leading cause of death for the nine countries at the turn of the millennium. However, it had become the second leading cause behind cardiovascular disease in six of the nine countries by 2016.
Realizing the problem in MEA
The IHE’s report underpinned the UICC’s three-year campaign for World Cancer Day that commenced this year with the theme ‘Realising the Problem.’ The first year of the campaign focuses on acknowledging the inequalities of cancer care around the globe and raising awareness that this inequity cost lives.
“The research highlighted that those countries that invest more in healthcare have better cancer survival rates for their populations.” – Thomas Hofmarcher, Health Economist at IHE.
Key MEA Cancer findings
So why is the MEA region particularly at risk?
It starts with awareness, realizing the problem, and then accessing the right cancer treatment services. The data shows that access to cancer care is limited in low-income countries.
Less than 30% of low-income countries have access to the right cancer treatment services. This is compared to 90% in high-income countries. In fact, an estimated 70% of deaths caused by cancer occur in low-to-middle income countries (LMICs).

Image credit: Hoedspruit Training Trust, South Africa
Access to cancer care services in MEA is a major issue
- An approximate 30-50% of all cancer cases are preventable, but it is the phenomenal gap in access to cancer care that is proving challenging.
- For example, 90% of all LMICs do not have access to radiotherapy, an essential method of treating cancer. Furthermore, a mere 5% of global resources for cancer prevention and control are spent on LMICs.
- The UICC also states that by 2040, the global demand for cancer chemotherapy will increase from 10 million to 15 million – two-thirds of which is expected to come from patients living in LMICs.
“It means that cancer is set to become the number two cause of disease burden in the MEA countries.” – Thomas Hofmarcher, Health Economist at IHE.
Which cancer is most prevalent in MEA?
Breast cancer was the most common type in all countries except in Egypt, where it was the second most common type.
Colorectal cancer was in second or third place in six countries, whereas lung cancer was in second or third place in four countries.
Thyroid cancer was in third place in the three Gulf countries (Kuwait, Saudi Arabia, UAE).

Image Point Fr/Shutterstock
Differences between men and women
Cancer rates and severity vary between men and women. Here is a snapshot of MEA:
Men:
Among men, the most common cancer type was prostate cancer, with a share of 14% of all diagnosed cases. Lung and liver cancer came in joint second place with a share of 12% each. This was followed by colorectal and bladder cancer, each contributing to 8% of all diagnosed cases.
The high share of lung cancer is associated with high smoking rates (see section 4.3), while the high share of liver cancer was influenced by high rates of hepatitis C in Egypt.
Women
Breast cancer was by far the most common cancer type for women, with a share of 33% of all diagnosed cases. The second most common type was cervical cancer (9%), followed by colorectal cancer (6%).
Cervical cancer and HPV
The high share of cervical cancer is partly driven by South Africa. The start of cervical cancer screening programs in some MEA–9 countries might also have led to higher detection of cases compared to other cancer types.
Cervical cancer and HIV/AIDS and human papillomavirus (HPV) in South Africa
South Africa has one of the highest prevalences of HIV/AIDS in the world. Causes of the high infection are of both biological and social nature. This includes a lack of awareness at the individual level on how to prevent getting infected, leading to unprotected sexual intercourse, gender–based violence, and poor protection of highly vulnerable key populations such as sex workers, in conjunction with inadequate provision of treatment by health care services.
The prevalence of HPV is high in South Africa in general, and especially high among HIV–positive men and women. This is because HPV is also transmitted through unprotected sexual intercourse. HPV infection is the prime cause of cervical cancer. Co–infection with HIV increases the risk of developing cervical cancer.
In 2000, a nationwide cervical cancer screening program was initiated. The government also implemented a national HPV vaccination program for girls in public schools in 2014.
HIV Aids impact
HIV/AIDS is linked to different cancer types. These include cervical cancer, anal cancer, non–Hodgkin’s lymphoma, Hodgkin’s lymphoma, Kaposi sarcoma, and conjunctival cancer. South Africa has nowadays the largest antiretroviral therapy program in the world. The country offers treatment and fights the spread of HIV. HIV/AIDS has now become a chronic condition, with patients leading normal lives. However, as a result of people living longer with HIV, the incidence of HIV–related cancer types is increasing.
 Breast cancer in MEA remains a major problem despite global awareness campaigns
Breast cancer in MEA remains a major problem despite global awareness campaigns
 Breast cancer in MEA remains a major problem despite global awareness campaigns
Breast cancer in MEA remains a major problem despite global awareness campaignsThe overall increase in cancer incidence between 2000 and 2018 was also shared by an increase in incidence in some of the major cancer types.
Breast cancer incidence shows a clear increase in all countries.
The development of lung cancer was relatively stable between 2005 and 2015 in most countries. By contrast, colorectal cancer incidence has been increasing throughout the entire period in all countries except in Jordan, where it was stable.
Thyroid cancer is the fourth most common cancer type (5%). On a worldwide level, women are about three times as likely as men to be diagnosed with thyroid cancer. However, the reason for this disparity is unclear and, importantly, there are no differences by sex in mortality from thyroid cancer.
The report provides detailed insights by country, age, and even mortality rates by cancer, age, and by country. There are clear differences.
The improvement of screening programs is critical
The report urges the improvement of screening programs. These programs, for breast cancer, cervical cancer, colorectal cancer, and prostate cancer have been implemented to varying extents in all MEA–9 countries.
The experience from other parts of the world shows that increasing use of screening for breast cancer and especially screening for prostate cancer can lead to the detection of cases of latent disease that never would have become symptomatic.
More lives can be saved in MEA
More focus is needed by private and public stakeholders in MEA on cancer care.
- Increase awareness of the first signs of cancer in the region.
- Physicians, nurses, and other health care providers need to be educated to recognize the symptoms of cancer.
- The public needs to learn about common symptoms of cancer. Awareness campaigns on symptoms (and on the opportunity of screening, if available) can increase the health literacy in the population.
Is it possible that underreporting is influencing the statistics?
Underreporting of newly diagnosed cancer cases has indeed been a persistent problem in the MEA-9 countries explains Dr. Thomas Hofmarcher . He says; “Some countries, such as South Africa, have made great efforts to improve this. In South Africa, the latest numbers from the Ekurhuleni population-based cancer registry are believed to provide reliable data that are representative of the whole country. By contrast, in Saudi Arabia underreporting is still a major issue. For a long time, the reported number of newly diagnosed cancer cases was around 50 cases per 100,000 inhabitants in Saudi Arabia, but the true numbers might have been closer to 100 cases per 100,000 inhabitants, similar to other countries in the region.”
“Growth projections are partly affected by underreporting. As noted in the report, future cancer numbers might almost double between 2020 and 2040 due to the expected demographic changes in the MEA-9 countries. The question is really from what base level do we expect the doubling to happen. It is very different if cancer cases double from a base level of 50 cases per 100,000 inhabitants to 100 cases per 100,000 inhabitants, or if they double from 100 to 200 cases per 100,000 inhabitants.”
In closing
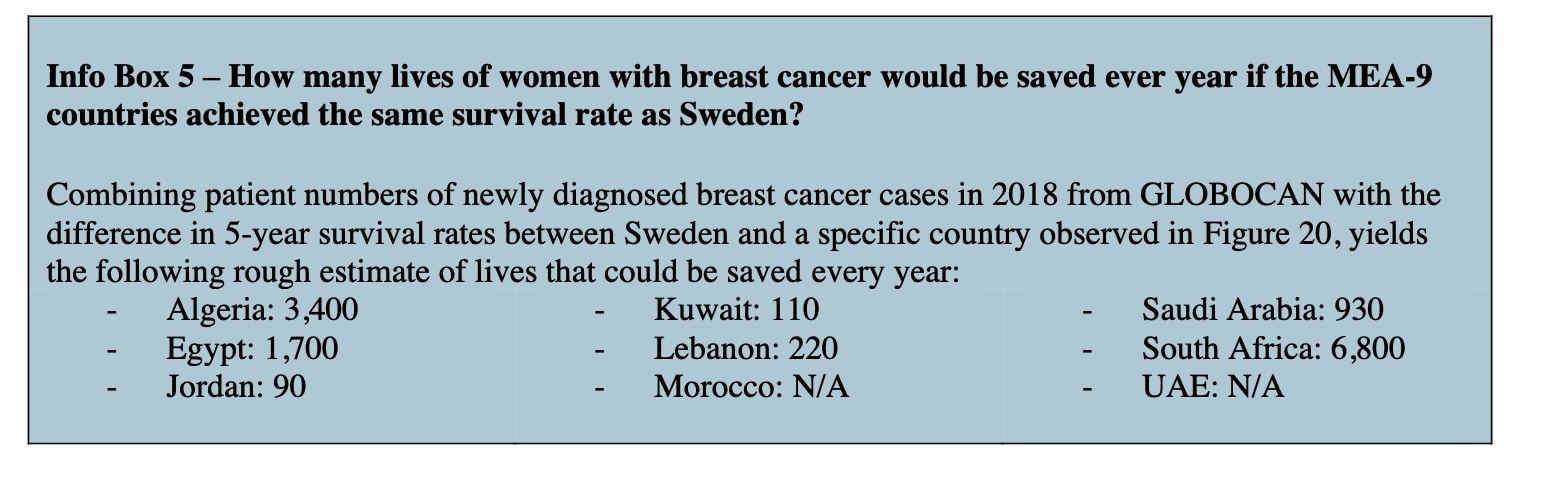
In closing, death from cancer can be reduced by MEA. As the following information visual shows. Many more lives could be saved with the right prevention, screening, and care.
About Lead author Thomas Hofmarcher Health Economist at SIHE

Dr. Thomas Hofmarcher is a health economist at the Swedish Institute for Health Economics (IHE) and scientific lead on the MEA study.
A core focus of his work is the comparative analysis of health systems and cancer policies around the world. He has led several major international projects on cancer care, studying access to cancer drugs as well as calculating the economic costs of cancer. His work on cancer has resulted in several research articles, policy reports, and book chapters.
While most of his earlier work focused on Europe, recent and current work also covers the Asia-Pacific region, and the Middle East and Africa – MEA. His research has been covered extensively in international media. He is also a regular speaker at international policy events and workshops.
References
Extracts from the study were used for this article. The study Cancer Care in the Middle East and Africa Hofmarcher T, Ahmad A, Lindgren P, Wilking: https://ihe.se/en/publicering/cancer-care-in-the-middle-east-and-africa-2/
The report was commissioned and funded by the PhRMA MEA Oncology Working Group and is based on independent research delivered by IHE. The PhRMA MEA Oncology Working Group has had no influence or editorial control over the content of this report, and the views and opinions of the authors are not necessarily those of the Oncology Working Group.
The Swedish Institute for Health Economics (IHE) was established in Lund in 1979 and is the first health economics research center in Sweden. This highly regarded research institute specializes in health economic analysis, medical science, and statistics. With close ties to Lund University and Karolinska Institutet in Stockholm and a team of highly skilled multi-disciplinary specialists, the centre delivers premium quality research and expert consulting within the healthcare field.
![women [longevity live]](https://longevitylive.com/wp-content/uploads/2020/01/photo-of-women-walking-down-the-street-1116984-100x100.jpg)